
More cases/less death?
More cases/less death?
Now we will see if the vaccines have impact

Cases are going up where I live. So are hospitalizations, including ICU admissions. What I haven’t seen so far is a significant rise in COVID-19 related deaths—but there is often a lag.
Just to recap—as we have seen this last year, hospitalizations lag cases, and deaths lag hospitalizations.
Over the last 3 months, two things are happening—people are getting immunized and variants of concern (VOCs), especially the B.1.1.7 variant first described in the United Kingdom, are rising fast as a proportion of new cases.
As many know, the vaccines directed against SARS-CoV-2, the virus that causes COVID-19, were evaluated on their basis to prevent disease, not transmission. The first two vaccines were largely evaluated in the US during a period when so-called “wild type” virus was extant. Wild type refers to the first broadly spread strain of virus. Now we are seeing different VOCs, especially B.1.1.7, displace wild type virus. How well these originally approved vaccines work against these variants is not fully known, but “vaccine breakthrough” cases are accumulating, and being reported across the country. Most of these are asymptomatic or minimally symptomatic. This bodes well for the notion that the vaccines will still provide protection against the most serious forms of disease in those who have been vaccinated.
The goal of vaccination, at least in these early months, was always focused on “immunizing for impact”, not reducing transmission. Initial recipients of vaccine were frontline healthcare workers and the highest risk individuals of having fatal outcomes. These are NOT the high transmission groups. The targeted impact is to PREVENT DEATH.
The highest transmission groups are the young adults who are least often symptomatic, thus most likely to unknowingly transmit disease to others.

As shown in the graph above, the highest number of cases per 100,000, starting with the summer of 2020 wave, and continuing into the fall and winter waves, was in the 18-24 age group, followed by the 25-44 year age group. Had the intent of vaccination been to decrease transmission—these would have been the age groups to target. In March and April of 2020, testing was extremely limited, and usually done on people who were symptomatic—the older age groups. Thus the higher numbers in older people early in this graph is an artifact of testing limitations.
The CDC has advised that people who have completed their immunization series can congregate together. Does this mean that they are not likely to transmit disease to each other? Unknown for sure, but likely not. It does mean that should they transmit disease between each other, they are unlikely to get sick or die. This is an important distinction.
So now we are entering the spring 2021 wave of transmission, and if the vaccines have impact, we will see less mortality than we did in the previous waves. If the vaccines are impactful, ICUs will not become overcrowded.
Israel, the country farthest along in vaccinating their population, will give us a clue as to how far immunization will quell transmission.
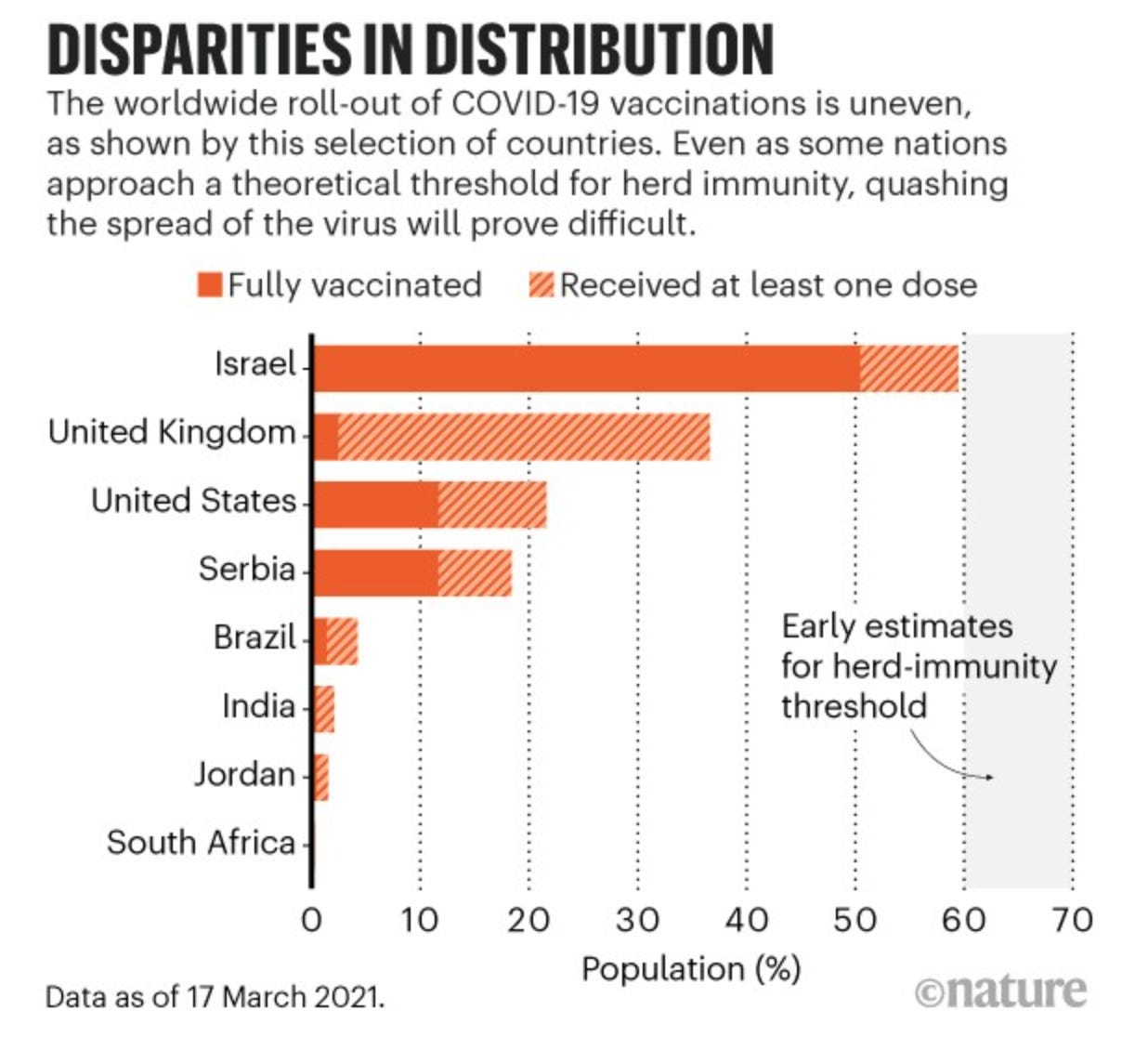
Nobody knows for sure what level of immunization and/or recovery from infection will lead to herd immunity. If recovered or immunized people can still catch COVID-19—and the vaccine trials show this happens at least 5% of the time, it may be that we never get to herd immunity. It is even more unlikely if people refuse immunization in large numbers. Should that happen, then SARS-CoV-2 will become an endemic virus, just like influenza and many other infections. In Israel, immunization rates have started to level off shy of the 60% mark.

At some point, our leaders will need to determine what normal looks like. Normal will likely include people continuing transmit, and to die from, COVID-19, just as they die from other infectious causes. Nobody is certain what level of transmission that will be.
However, thanks to the vaccines, most likely we may be able to live with COVID-19, and not die from it.