



Covid-19 is over--right?
It is--and it isn't. Depends on who, and where, you are.

The end is in sight. At least the end of the Public Health Emergency and National Emergency are planned to end on May 11, 2023, according to the White House. Most of us will be glad to see this gone. Back to normal. But it is not that the virus will disappear.
As people stop testing and reporting illness, for better or for worse, my go-to metric for evaluating level of virus remains wastewater testing of viral particles. We have a very robust process in the Twin Cities.

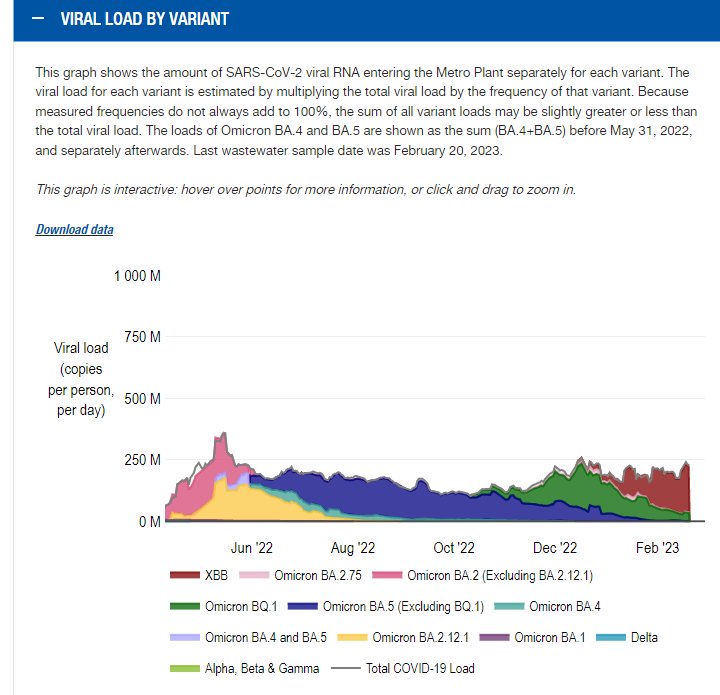
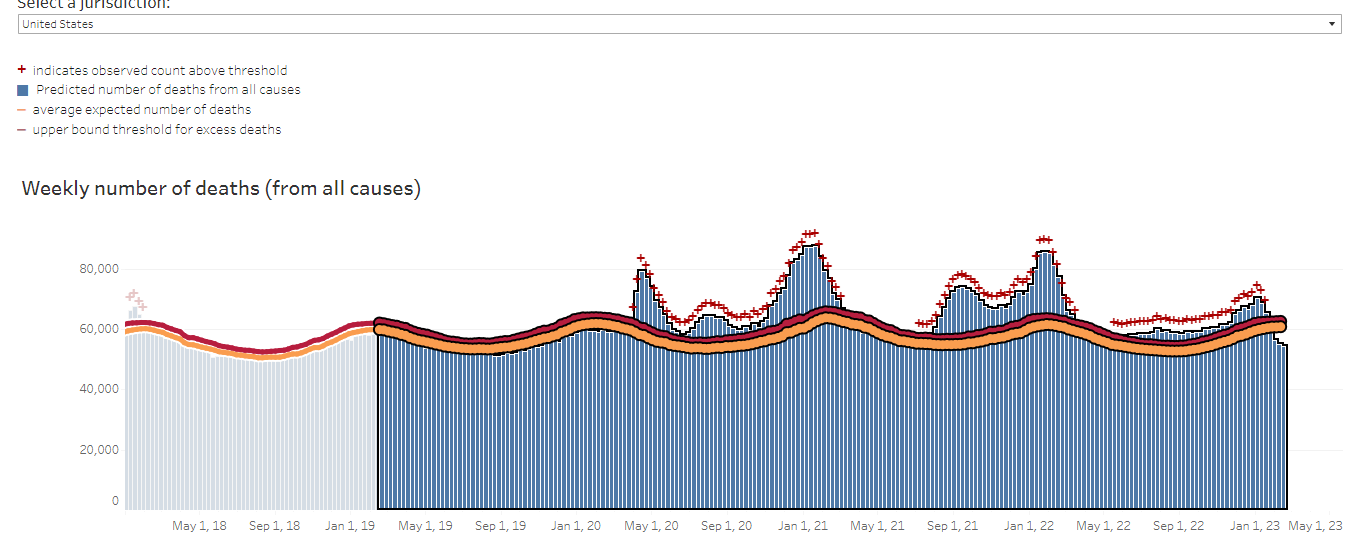
What I like about the wastewater data is that it is an unbiased collective measure of the amount of virus in the waste stream. It is not prone to gaming. “Everybody goes,” as they say. And while in prior years, the wastewater data correlated well with cases, there has been a disconnect over the last few months. Viral load has been going up over the last four months, but cases have been going down. That is a good thing. Part of it is likely due to decreased case testing, but much of it is likely due to decreased symptomatic cases. Excess mortality over this past fall and winter is starting to return to baseline—although we are not there yet.
So, indeed, we are through the worst of it, collectively, as a nation and a population.
Yet, I am still seeing people hospitalized and sick because of Covid-19 (not just with it—which is still pretty common) but actually sick from Covid-19. And the excess deaths would suggest that it is still a factor.
Almost everyone I am seeing sick because of Covid-19 has some “risk factor” for a bad outcome. Many are elderly or severely immunocompromised, such as organ transplant patients. This remains a fraught time for those patients, as the protective monoclonal antibody, Evusheld, is no longer effective against the predominant subvariants of Covid-19.
The good news is that the Covid-19 antivirals, paxlovid, molnupiravir and remdesivir, remain quite effective at preventing death. The key is to get started on them as soon as possible. For that to happen, testing and treatment have to be readily available.
Masking—is it worth it?
I have seen a lot of commentary about a study released by the Cochrane Collaborative about masking. They performed a meta-analysis of studies regarding the effectiveness of masks to prevent transmission of respiratory viruses. Before I address the conclusion of the studies, I would like to review what the Cochrane Collaborative does, why it is important, and what are the caveats.
The Cochrane Collaborative is a highly respected group that performs meta-analysis. They do not do original research. Instead, they collect research papers from other scientists, review the rigor of the studies, and provide their own analysis as to what the available evidence shows. They will discard studies that are weak in terms of data and statistical significance, and elevate studies that include the strongest possible techniques—the randomized controlled trial (RCT). If the Cochrane Collaborative says an intervention is effective, it means it has passed the highest level of review. For example, they concluded the Covid-19 vaccines are highly effective and safe.
However, when the Cochrane Collaborative says the data does not show effectiveness, it does not mean that the intervention is not effective—only that the available data does not show effectiveness. The studies may have been poorly designed, lack statistical significance or have other errors that limit the ability to show effectiveness. That is not the same as describing something as ineffective or even dangerous.
So what was the conclusion about masks? Just that the data available to date does not show masks are effective at preventing transmission. The authors concluded, “The high risk of bias in the trials, variation in outcome measurement, and relatively low adherence with the interventions during the studies hampers drawing firm conclusions.” Plainly—we need better designed studies.
My experience has been that masks do reduce transmission. Probably the best evidence I have seen is in hospitals. We saw clusters of transmission between healthcare workers in the one setting where they did not wear masks—break rooms. Everywhere else, healthcare workers have been masked while in the hospital.
Masks remain an important part of the “Swiss Cheese Model” of preventing viral transmission, as explained by Prof. Ian Mackay:

Any single intervention may be weak by itself, but when applied with other interventions, and consistently, it can reduce viral transmission. I wear masks less than I used to while out in public, but will continue to do so in certain settings—including sitting next to strangers on airplanes.
Appreciate the insight. Well written. Thank you
Thank you Dr. Bornstein : you are an excellent teacher and clinician 🙏😎